Splayfoot problems
Metatarsalgia, ball pain, arched splayfoot
Due to the weakening of connective tissue, excess length of metatarsal or due to other biomechanical factors, middle-aged and elders may experience severe pain at the ball of the feet. If a conservative treatment with special inserts and other measures does not help, then an operation is often the solution.
The aim of surgery is to withdraw the metatarsal head from the weight-bearing zone by shortening the metatarsal.
We disagree with this, because the disadvantages outweigh:
Common and widely used is the so-called Weil-surgery.
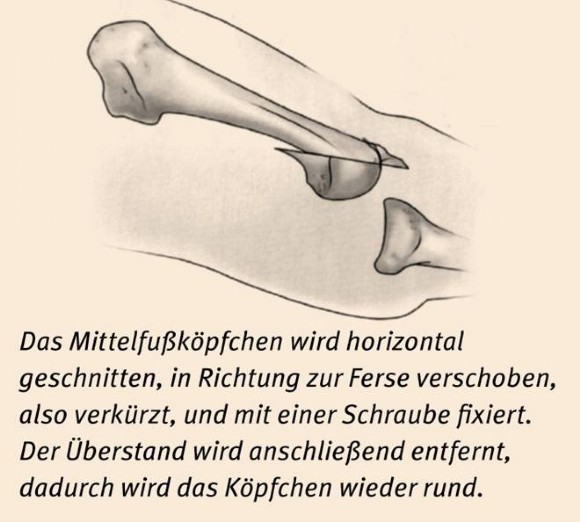
Bone is taken from the metatarsal head and the metatarsal head is moved forward towards the soles, parallel to the heels, and thus the metatarsal is shortened (fig)
The operation certainly has its advantages, it is done quickly and helps to eliminate the ball pain.
Yet, healthy cartilage and bone tissue is sacrificed in this procedure, there is now an inevitable unevenness in the middle of the toe joint, and thus sooner or later (perhaps after years) a restriction in movement and osteoarthritis (a degenerative joint disease) can be caused.
The metatarsal head is cut horizontally, moved in the direction of the heel, thus shortened, and fixed with a screw. The supernatant is then removed, thus the head is round again.
Operation according to Weil, which can often cause problems.
Here's an example:

The surgery according to Weil is also very error prone. This elsewhere performed Weil-operation shows very long screws that burrow into the plantar plate (red arrows). Screws, which are not functional outside of the bone (arrows). Poorly rounded head and periarticular screw position (yellow arrow), which hinder the mobility of joints and lead to early osteoarthritis.
But even the most perfectly executed operation inevitably leads to problems, limited mobility and arthritis due to the cutting through of healthy cartilage and bone tissue.
What we do - modified method: DMO
For this reason I have developed a modified method of metatarsal shortening since 2005, that uses a bone cut behind the cartilage area. The surgery is called DMO distal metatarsal osteotomy.
Using a careful bone-section that preserves all the important structures, it is possible to restore the necessary metatarsal parabola (alignment), without sacrificing healthy cartilage and bone tissue in the joint and without having to create unevenness.
This bone cuts cannot be done "free hand". We have therefore developed precise guides that will help the cuts be done effortlessly and precisely. They are fixed with our V-tek screw.
An example:

Left: Very long III metatarsal, pain and callus formation. Please note the "bump" at the II metatarsal : The poorly performed hallux operation became a burden on the metatarsal bones. The II broke and itself "fixed" the problem. The III. remained whole but further painful.
Right: After shortening the metatarsal III pain was gone very soon, the callus on the soles decreasing.
Here is another example, with a drawn "metatarsal index" (or parable or Alignment)


Left: the metatarsals II, III and IV are too long and do not make the necessary parabola, which results in too much burden, pain and calluses in the ball area.
Right: So it should be: After the operation, the X-ray shows the metatarsals. The I metatarsal is the longest, the II is about the same length or slightly shorter, the III. even shorter, etc.

The pain and calluses disappear after a short time:
Left: before surgery / Right: after surgery
Another example:

After an elsewhere conducted, improper hallux surgery with shortening of the metatarsal I, the II, III. and IV bone became relatively lengthier, shown here by the yellow lines.
The patient suffered from massive splay problems that were not controllable with conservative measures. Therefore, a further operation had to be carried out. The red lines show the planned shortening in the re-operation.


Both feet had to undergo a shortening of the metatarsals. The parable was achieved and the splayfoot problems disappeared after a short time.
Currently we provide the distal metatarsal osteotomy unfixed and use only stab incisions of 2 or 3 mm. This gives us a rapid healing, less swellings and less pain.