Hallux Valgus
(Hallux valgus, "Bunion", deviation of the big toe)
Read also: "Hallux philosophy"
Definition
This deformity of the forefoot is the most common foot disease. The big toe increasingly deviates from its straight positioning in the outside direction. The toe stands away from the midsection of the body. The foot gets much wider due to the strutting apart of the first metatarsal and you can see a more or less great curvature inside, at the big toe joint. This strutting apart is, in connection with the pull of the tendons, the main cause of the hallux valgus deformation.
Usually the deformity does not cause any pain initially, but only shoe pressure problems when wearing tight or hard shoes. Later, when the big toe joint also consists of an abrasion component, or when bursitis set about the bunion, strain and rest pain emerge. The development of hallux valgus is reinforced by bad (sharp) footwear, high heels, overstressing, weak tissue, hormonal and other factors. It affects mostly female patients and has a strong genetic (ie hereditary) component.
Correction
The correction of hallux valgus should take place sooner rather than later, because milder forms with an intact joint can be corrected better and more lasting than later stages. The medical literature shows more than 150 different procedures to correct this misalignment and it therefore goes without saying that none of the methods can be applied for all forms of the deformity. Some of the methods have (especially in combination with others) emerged as the "gold standard", a good surgeon therefore needs to be familiar with 5-6 surgical procedures very well.
The V-tek method
Not entirely happy with the current methods and convinced 100% by any of them, I have tried since 2003 to improve the methods and develop new ones. These new and improved methods which have led to the development of new implants, have been proven to be successful after many trials and are now routinely used with great success for patients.
Below I present the various surgical procedures that are used in our center.
1. Mild to moderate hallux valgus - IM angle up to 14 degrees
The deviation of the big toe to about 30 degrees and the strutting apart of the first metatarsal from the second metatarsal is not more than 14 degrees. In addition, the big toe joint may possibly not be congruent, meaning that the joint partners do no longer fit together optimally.
The essence of the operation is a combination of soft tissue and bone correction section under the head. The correction of those feet is done with the so-called small V-tek plate. This implant is made of titanium, and 30 mm long. Fixation is done - depending on the model - with 3 or 4 screws with a 2.7 mm diameter. The plate was developed for this most common form of hallux valgus. The operation will be carried out minimally invasive with average cut lengths of 8 to 15 mm. Additionally we employ 2 or 3 stab incisions of 3 mm length. Patients can resume normal activity immediately after surgery.
The advantages of the in-bone fixation technique are:
- The forces are retained where they occur
- The metal does not bother because it is inside the bone
- There are a lot more correction options available, than with conventional surgery
- The toe and the metatarsal heads can be adjusted in 4 levels: to the middle of the foot, to the bottom, rotating and improving the joint angle.
- No loss of length of the first metatarsal, therefore, no overloading the other metatarsal heads
- Usually no metal removal required
- Plates stay inside
- Immediate ambulation with full loading possible
Example I:

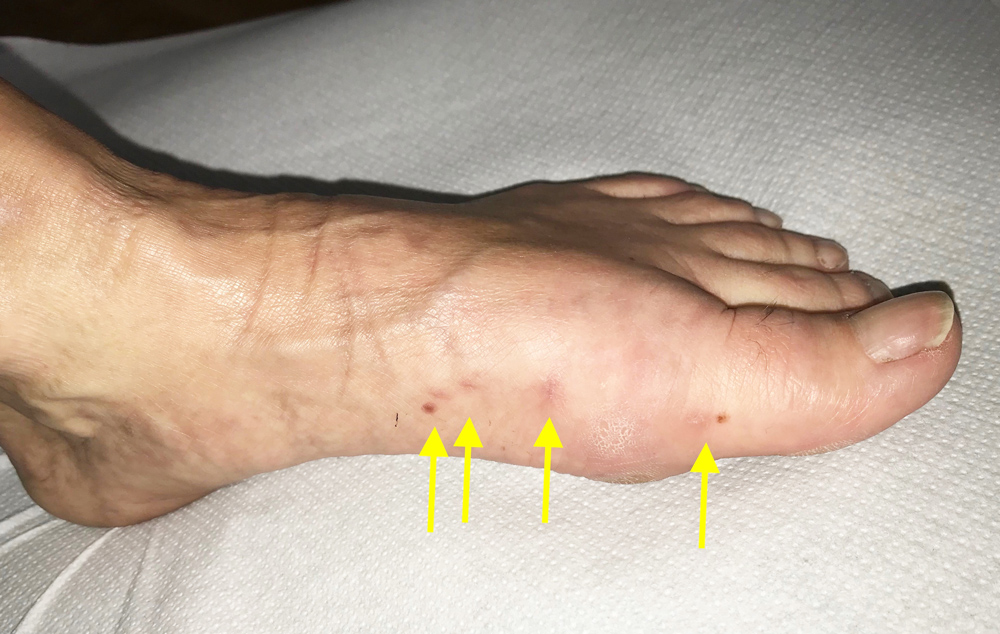

Patient K (female, 51 years) before and 8 weeks after the percutaneous surgery. The scars are very small and big toe is straight. The dark dots on the left and right side are not scars but moles.
Example II:

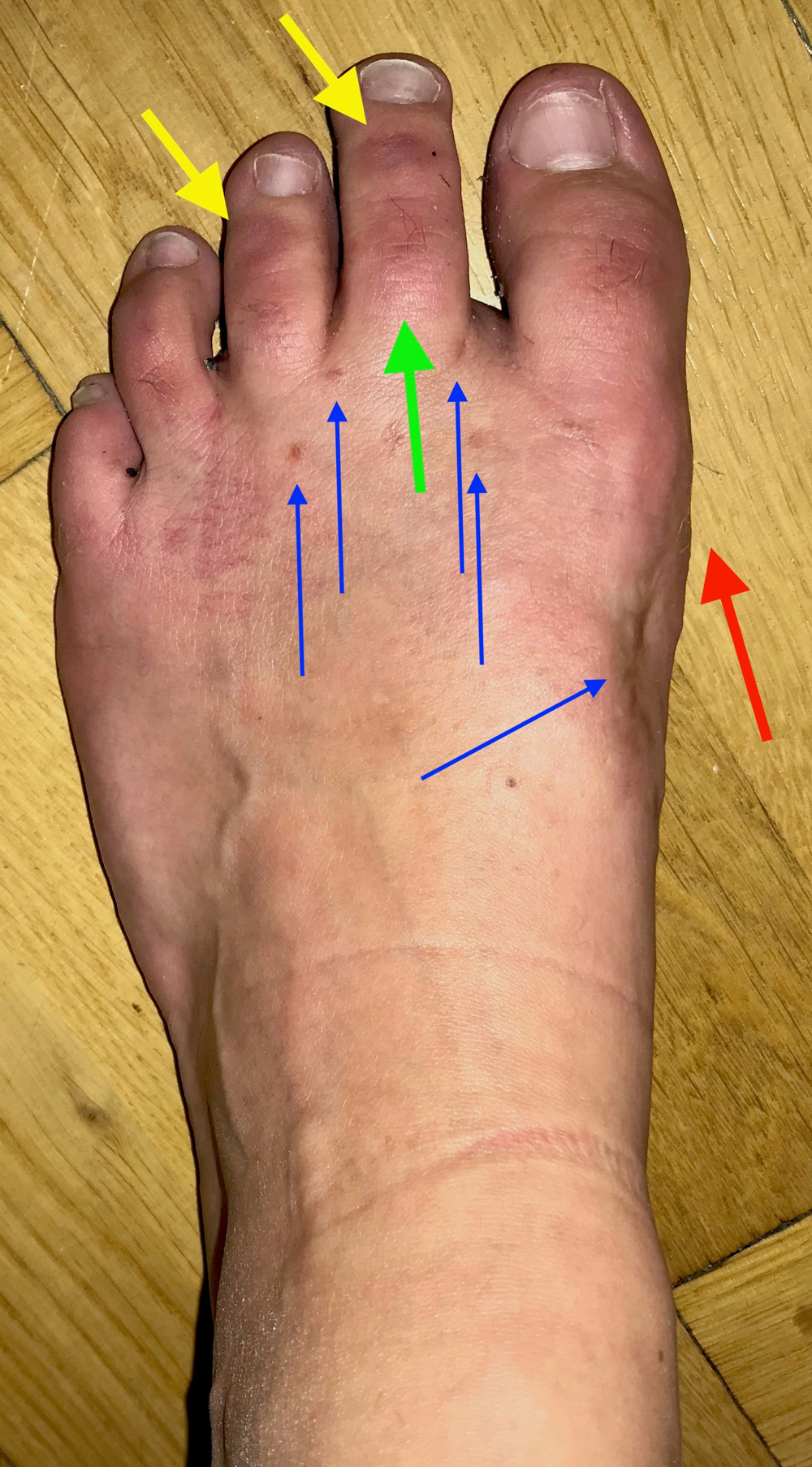
Before: Patient XY (female, 26 years) was operated 2 years ago by an other surgeon and was very dissatisfied with the result. The deformity recurred in a short time (red arrow) and additionally the 2nd toe developed a claw toe (green and right yellow arrow) and the 3rd toe developed a distal hammertoe (left yellow arrow).
After: 6 weeks after our correction. The big toe was permanently straightened (red arrow), the 2nd toe was was permanently straightened on the proximal (green arrow) and distal joint (right yellow arrow) und the 3rd toe at the distal joint (left yellow arrow). The scars are tiny (blue arrows). They will become invisible after a short time.
Unbelievably but true: The patient had never pain after the surgery and she still has no pain. The function of the foot is excellent.
Example III:

Before and 6 weeks after surgery. Incision length about 10 mm, the scar can be hardly noticed. The patient was able to resume her work after 10 days.
In the x-ray you can see the complete restoration of a normal joint situation. The red lines indicate the length of the first metatarsal. There is no (reduction) shortening of the 1st metatarsal after surgery, as happens frequently in other methods also leading to overload and pain in the other metatarsal heads. Material removal is, due to the titanium plate and titanium screws, no longer necessary.
2. Severe hallux valgus
IM Angle of between 14 and 18 degrees and stable TMT I joint
For these deformities is a minimally invasive surgery no longer suitable, since the deviations of both the metatarsal and big toe are already too strong. The medium V-tek intramedullary locking plate is used here and the bone cut is set at the base of the first metatarsal. In addition, a soft tissue correction is necessary.
All the above mentioned benefits apply here.

Left, before the operation: Shoe pressure discomfort and pain at rest. After surgery, beautiful, pain-free foot. Also note the correction of the twisted toes.
In the x-ray you can see the correction without loss of the first metatarsal length, thanks to the locking plate. The patient was able to resume full activity immediately after the operation. Material removal is not necessary thanks to the titanium plate.
3. Strong and very strong bunion
IM Angle over 18 degrees and/or unstable TMT I joint.
The spreading of the metatarsal I and II is very strong, the feet are really wide at the front, and fit only in very wide shoes. Mostly severe pain occurs.
The correction must be done relying on the first x-ray, by stiffening the mid-tarsal joint (cuneiform-metatarsal joint, TMT I). Here we use the same selfdeveloped technique. The long intramedullary locking plate (55 mm) is used. We use also in this procedure the minimally invasive surgical technique.
All before mentioned advantages are applicable for this technique.
Example I
A 52-year-old woman with massive shoe problems and pain before surgery.


Deformity before surgery, marked by the first x-ray. Ideal correction and narrow foot post-surgery.
The X-ray shows the amount of abduction before the operation and the narrow foot with parallel bones after surgery.
Beautiful correction and painless foot, long walks are possible after a short time. Material removal is not necessary, due to the titanium plate and titanium screws.
Example II
A 64-year-old patient with this complex deformity, metatarsal overload pain and hammer toe II.

Left before and right after the surgery: Very nice correction of this massive deformity of the entire forefoot.
Example III
A 42-year-old woman, waitress, because of severe pain when walking she couldn't work properly.

Her left foot before and after surgery. She could resume activity immediately after surgery, and return to her hard-work after 8 weeks. X-ray on the right side. Durable correction with the 55 mm V-tek plate. No shortening of the toe or the 1. metatarsal. No protruding wires. Plate removal is not necessary thanks to the titanium plate.
For more examples of successful Forefoot-correction please also check the