Upper ankle
The upper ankle joint consists of three bone forming units.
Mainly the shinbone (tibia) and the talus (astragalus) are involved in the joint formation, on the outside also the fibula forms a small portion of the joint with the talus.
As with all joints, the sliding surfaces are covered with a 3 - 5 mm thick layer of cartilage (hyaline cartilage).
Instability of the upper ankle joint
The articulating bones previously described are "held together" by a joint capsule and ligament structures more or less strong, at rest and during stress. Due to an injury to these ligaments, mostly to the outer sidebands (the typical tipping), an instability can arise.
While fresh injuries are treated mostly with a splint, the surgical treatment of chronic lateral ligament instability is described below (recurrent subluxation of the talus). Sometimes the instability occurs despite adequate initial treatment and treatment with the Malleoloc splint. The symptoms are pain, instability in walking and frequent tipping of the ankle to the outside, such as when walking down the stairs, stepping over a curb or while jumping.
Affected patients are rather young and increasingly women due to the less tight ligaments.
The diagnosis is made by a manual examination (clinical), and possibly radiographs by means of a so-called "fixed" recording, in which the dislocation mechanism is simulated, such a recording is usually painful and therefore dispensable.
Treatment principle
The so-called periosteum plastic is applied, whereby plastic does not necessarily mean plastic, but rather replacement or regeneration.
The surgery is performed using a skin incision approximately 10 cm long. By peeling, folding down and attaching a strip of leg skin, it is possible to strengthen or replace weak or torn ligaments.
Unlike other common methods, the replacement ligament is attached to the anatomically correct places (which is not always possible with a tendonplasty), and thus does not lead to a mobility restriction of the other foot joints.
A long untreated instability of the upper ankle is bound to cause early abrasion (osteoarthritis) of this joint.
Aftercare
Postoperatively, a lower leg lay-cast for two weeks and then a walking cast for another three weeks will be used.
The lower leg cast does not necessarily mean that the patient only has to rest, but he can walk using two forearm crutches to relieve the operated foot. A walking cast can be fully loaded.
After cast removal, physiotherapy is performed to recover the strength and mobility.
Ability to work
Office work can be resumed, if necessary, after a week on crutches and lay-cast, otherwise after two weeks with the walking cast. Heavy physical work can be allowed after two to three months.
Sports ability
Foot straining sports such as tennis and squash should be resumed only after about four months, cycling, swimming and running can be started cautiously after ten to twelve weeks with the use of appropriate footwear.
Results
In about 92 percent of the cases, a good result can be achieved in terms of stability and mobility.
In about 15 percent, a certain limitation of physical activity can be expected.
Complications
In about 2 percent, a (usually temporary) sensory disturbance can occur on the outside of the foot.
A dreaded complication of any surgery is the infection, which makes treatment with antibiotics and sometimes a further surgery necessary. Fortunately it occurs very rarely and is usually well controlled so that though the healing process is delayed, the end result will not be affected. The infection occurs in less than 2 percent of the cases.
In 1 percent of the cases, ankle movement restrictions of 10-20 degrees remain. In about 2 percent of the cases (but often after a new injury) a renewed instability in the upper ankle joint occurs.

The newly formed bands are attached to the strong threads, which are anchored in the bone with bone anchors. Alternatively, screws with washers can be used.
Diseases in the interior of the upper ankle joint
Diseases, disorders and injuries of the inner joint area may affect the articular cartilage, the underlying bone, the bands or the synovial membrane, which lines the inner capsule. They can all be diagnosed, treated and prognostically assessed arthroscopically.
The complication rate in arthroscopic surgery of the ankle is almost at zero percent.
For the patient, the procedure is minimally burdensome, and represents a major advancement compared to the open surgery, in regards to postoperative pain, healing time, length of hospital stay and complications.
For the operator, this method is demanding regarding experience, patience and skill.
With the introduction of high-frequency surgery, a further improvement of the results has been achieved.
Loose joint bodies
Due to injury or local hypo-perfusion, cartilage-bone parts can be stripped off from one of the three joint surfaces and can cause discomfort as a free body ("joint mice").
The complaints are often very diverse:
- Rest and/or stress pain
- incarceration symptomes (ankle block)
- swelling and irritation.
The diagnosis is made radiographically or possibly by magnetic resonance imaging.
Treatment principle
Arthroscopic removal of loose bodies under general anesthesia or local anesthesia.
Aftercare
No post processing, getting up on the first day after surgery.
Working and sporting ability
Both are possible after a week-ten days.
Results
Is there no other damage in the joint, can a 100% success be expected.
The success is lower, the more there is damage present in the joint.
Example:
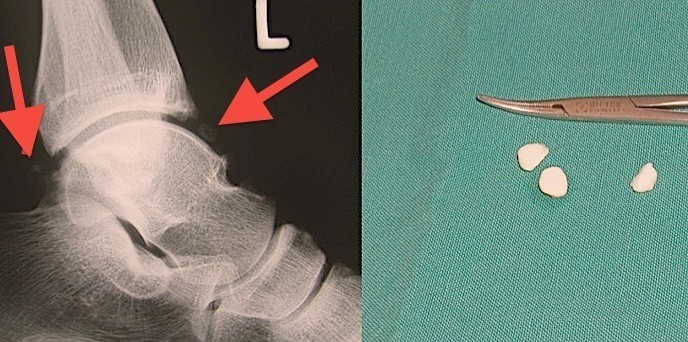


Left: Small free joint bodies in the upper ankle joint (arrows). After an arthroscopic removal you can see the size of the cartilage-bone pieces.
Middle: In this case, we were amazed at how many pieces of cartilage there were in the ankle joint. The X-ray shows almost nothing.
Right: The removed chondroma.
Osteochondrosis Dissecans (OD)
Osteochondritis dissecans might be regarded as preliminary stage of the loose joint bodies.
Due to a local hypo-perfusion (possibly caused by injury), usually at a typical point of the ankle bone (talus), a piece of cartilage-bone is stripped off. (osteochondral).
The disease progresses in four stages, which can be assigned with various symptoms (see table).
The OD usually affects younger patients and more often men than women. The diagnosis is made radiographically and by magnetic resonance imaging (MRI).
Stages of OD:
- Stage I: Radiographically recognizable bone densification, chondromalacia (MRI), usually no pain, irritation possible
- Stage II: Partial cartilage bone detachment. Pain caused by the protruding cartilage part: Irritation, swelling
- Stage III: a total release of the dissecate (cartilage bone piece), but it remains in its place. As stage II, possibly severe rest pain.
- Stage IV: The dissecate leaves his bed and mostly becomes a large free body. Severe pain injection, swelling, joint blockage.
Treatment principle
Osteochondritis dissecans in stage I require no treatment when symptom-free. In case of pain, a sports ban and immobilization can lead to success.
If therapy-resistant a "reconnection" of the dying bone is made with the vascular supply, by means of an arthroscopic drilling.
In stage II, protruding cartilage pieces are removed arthroscopically and the osteochondral drilled back on.
In stage III, the osteochondral (free piece of cartilage bone) is reattached to his "bed". For this we use small screws or pins, which are inserted arthroscopically (or openly).
In stage IV the mostly large free body is removed and its "bed" smoothed. Often a synovectomy (removal of the inflamed inner joint skin) must be performed in addition, regardless of the stage.
Aftercare
In stages II to IV, the operated ankle joint is only to be partly loaded, for about four to six weeks (forearm support crutches).
Ability to work
Office work after five days, hard labor after six to eight weeks, depending on the stage.
Sports ability
Light sports after about four to six weeks, heavy sports after three months.
Results
Depending on the stage, a chance of recovery to about 90 percent can be achieved.
Complications
In stages II and III, the free piece of bone can die, so it can not be united with the rest of the talus. It must then be removed in a second intervention.
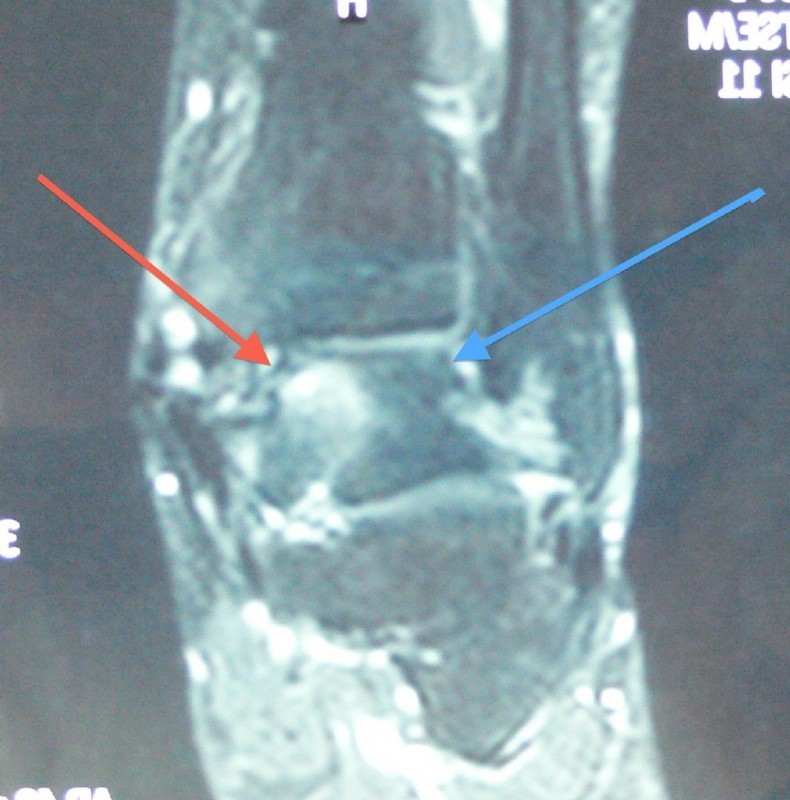
The red arrow shows the typical localization of an OD, which does not occur after an accident. One sees a brightening (bone edema, fluid retention). This is stage II.
The blue arrow indicates the localization of a OD, which occurs after an accident.
Inflammatory changes (rheumatoid, after injuries)
Degenerative changes (abrasion, injury consequences)
Non-specific pain and swellings
Although these diseases can have very different causes, they are summarised under this topic. It makes sense to discuss them together as all are treated using arthroscopical surgery.
The inflamed synovial membrane, regardless of whether it is rheumatoid, degenerative or even caused by bacteria, may be removed arthroscopically by vacuum milling and the radiosurgical probes (synovectomy).
Cartilage damage and arthritis can be smoothed using arthroscopical surgery or abraded (see stages and treatment of cartilage damage and the treatment of osteoarthritis in the knee section).
Caused by abrasion or frequent overuse of athletes, epiphyses on the shin and ankle bone can lead to pain and limitation of movement in the upper ankle joint. These border strips can be well removed arthroscopically, causing the pain and irritation to subside and the mobility of the joint increases.
The arthroscopy of the upper ankle has a very special role in the diagnosis and treatment of unknown pain, where no clarity could be found with other diagnostic or therapeutic procedures. These states (often due to injury) often show arthroscopic cartilage damage and/or inflamed mucous membrane areas or cicatricial adhesions, that are very well treated using arthroscopical surgery.
Aftercare
The post treatment is usually short (physiotherapy). Except after abrasion, immediate loading is possible.
The additional treatment after abrasion as a treatment of osteoarthritis of the upper ankle is similar to that of the knee joint.
The results are very good, but the exact prognosis depends on the individual case. Therefore, collective results can not be mentioned.
Using a radio frequency technology further enable improvement in the results, especially in the cartilage treatment, and in bloodless synovectomy (synovial membrane removal).



Left: Bone spurs in the front part of the upper ankle (on the shin and ankle bone) hinder the movement and cause inflammation and pain.
Middle: The vacuum miller removes the bone spurs arthroscopically.
Right: The result shows the newly acquired space. The pain is gone.
Operative ankle (Arthrodesis)
If the upper ankle is largely destroyed and severely painful due to injuries (severe fractures), osteoarthritis (wearing down) or inflammation, and not responding to conservative therapy, then a possible way is an operational ankle stiffening.
The patients often shy away upon hearing this word, because they think they can then no longer walk properly. Mostly, however, exactly the opposite is true.
By eliminating the pain, with proper management of the operation, the patients can afterwards walk so well that other people do not even notice the "disability". The role of ankle stiffening is certainly taken lightly due to the improvement of the alternative methods (TEP, sliding surface replacement - see below). The stiffening is, however, still the most reliable, but both in a positive and negative sense, a "definitive" method.
Treatment principle
Arthroscopically or openly, the damaged joint surfaces are removed and the bone surfaces "freshened", so that a healthy bleeding bone (cancellous bone) comes to light.
Then both parts (tibia and talus) are combined by means of a bone assembly (osteosynthesis).
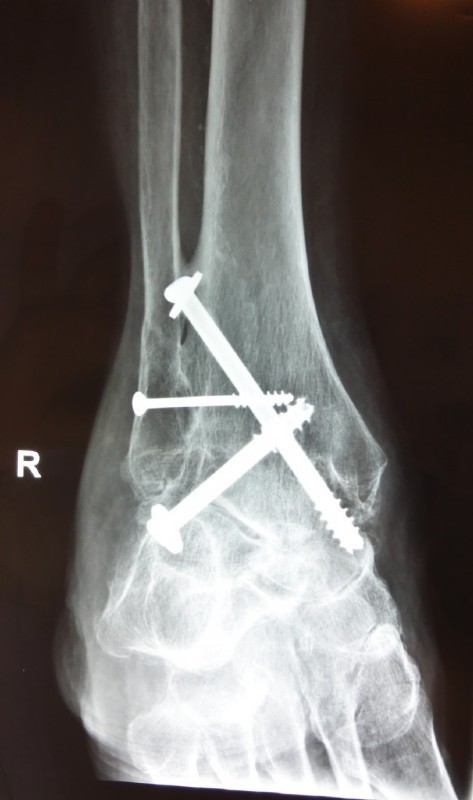
We use diagonal screws for osteosynthesis.
Aftercare
Postoperatively, a lay-cast (relief with two forearm support crutches) is applied for six weeks and then switched to a walking cast for another six weeks.
After cast removal an orthopedic shoe may be necessary.
Ability to work
Office work after six to eight weeks with a walking cast. Heavy physical activity is possible in exceptional cases, after about four to six months.
Sports ability
Cycling and swimming about three to four months after successful bone healing. Other sports should be discussed with us first.
Results
In about 90 percent of the cases, freedom from pain and a satisfactory gait is the result.
Complications
In about 8 percent the bone parts do not connect (nonunion) and require a re-operation.
The infection rate is less than 1 percent in an arthroscopic surgery, in the open method at 3 percent.
In very few cases (no such case with our patients) the vessels or nerves are injured or thrombosis may occur.



Artificial ankle (Total hip, gleitfächenersatz, joint replacement)
Treatment principle
As with all other joints, the used up cartilaginous sliding layer is removed frugally with the underlying bone and replaced by a metal-plastic combination at the upper ankle.
The special feature of the latest generation of these prostheses is, that a floating plastic plate lies in between the two anchored (cementless) metal parts in the bone. Thus, it is possible for this prosthesis to perform not only hinge movements, but also easy sliding and rotating movements – like a natural ankle. The load on the bone decreases and the loosening rate is thereby reduced.
Aftercare
Hospital stay about two weeks. Immobilization in the plastic splint or plaster cast for four to six weeks, followed by physiotherapy. Partial weight bearing after six weeks, full weight bearing possible after eight weeks.
Working and sporting ability
Light work and walking after three to four months. Heavy load, contact sports and running banned permanently.
Results
Good results in terms of pain reduction and functional gain in approx. 90 percent. Approx. 85 percent of the implants last for 10 years.
Complications
Infections in 2 percent, loosening of the prosthesis with a need to change or remove the prosthesis and joint stiffening in 15 percent of the cases(over a 10-year period). Rarely joint stiffness with the need for an operational solution. Rarely numbness of the foot and thrombosis.
Example:
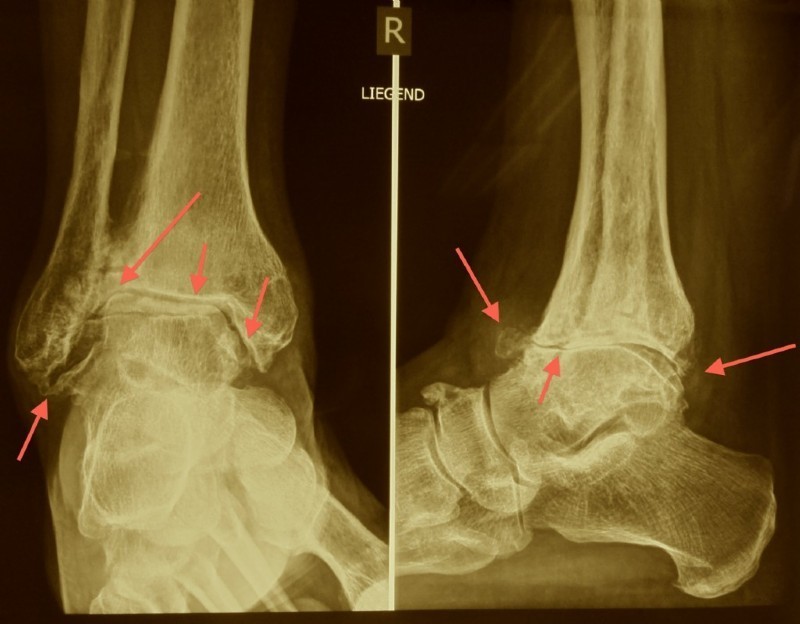
Very severe osteoarthritis of the upper ankle, the arrows show the bone spurs, joint space repeal and the new bone formation.




For this patient an additional outer ligament reconstruction had to be performed. We also had to temporarily remove the inner ankle and then screw it back because of the difficult circumstances.
The patient has been walking with it for 20 years now without pain.
A modern endoprosthesis (Hintegra) with additional treatment of a fibula fracture.




The feet of the patient with the Hintegra prosthesis, 6 months after surgery:
The mobility of the ankle is almost the same on both sides.
The inner and outer rotation of the heel works very well.
The video shows a completely normal gait six months after the operation:
Cartilage repair, autologous chondrocytenimplantation (ACI), cartilage transplant
At the upper ankle, it is also possible to repair cartilage damage. However, just as with the knee, not the entire cartilage surface should be destroyed, but only small-to medium-sized defects can be closed with new cartilage. For more information, please refer here.