Achilles tendon
The Achilles tendon is the largest tendon in the human body.
Enormous force is transmitted from the lower leg or the whole body to the foot. Force potentiation occurs through sudden running or jumping. Due to its vulnerable position, injury of the Achilles tendon and acute and chronic afflictions of the tendon and its enthesis on the calcaneus is frequent.
Achilles tendon injuries
Achilles tendon injuries are strains or in more severe cases tears. Strains usually do not require treatment; tears however must be treated surgically. The best prognosis is on fresh, partial tears, which are treated in a timely manner.
Old complete tears, where the tendon ends have already retracted, can sometimes cause major problems, especially since these injuries result from degenerative conditions under which the Achilles tendon was already damaged. The Achilles tendon is then thickened, fatty tissue is deposited, and the quality of the tendon fibres decreases. Tendons such as these tear more easily than healthy ones. The ends of the tendon are then already very frayed and defibrated.
In order to bridge the defective area, either artificial tendons must be implanted or a part of the healthy, remaining Achilles tendon must be lowered to bridge the defect. Both methods require a relatively long immobilization period of 8 to 12 weeks.
Example:
A patient with long term heel pain and increasing disability to walk despite conservative treatment. After closer examination, a chronic rupture of the Achilles tendon was found.

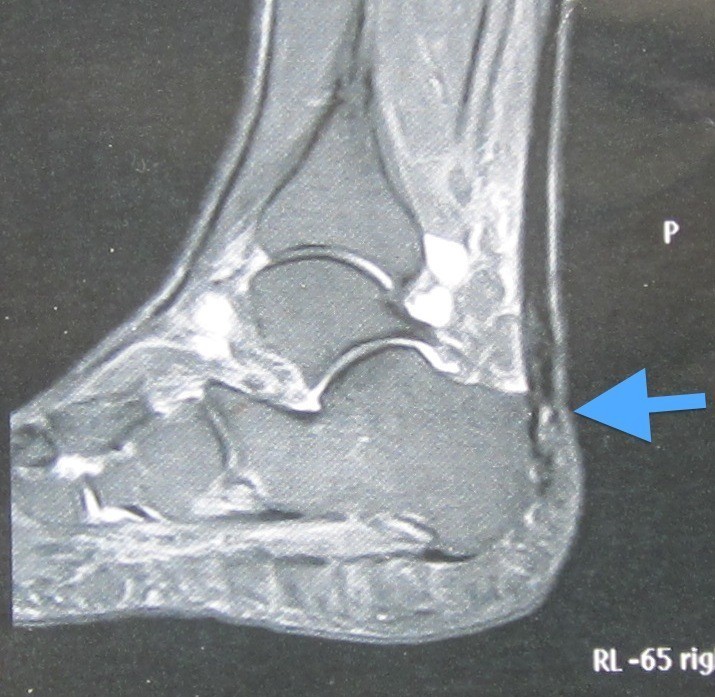
On the X-ray and MRI can be seen that a piece of bone was also torn off with it. The cause was an upper calcaneal spur that broke off.
The conservative treatment carried out elsewhere was stopped by us immediately and the patient was operated on:
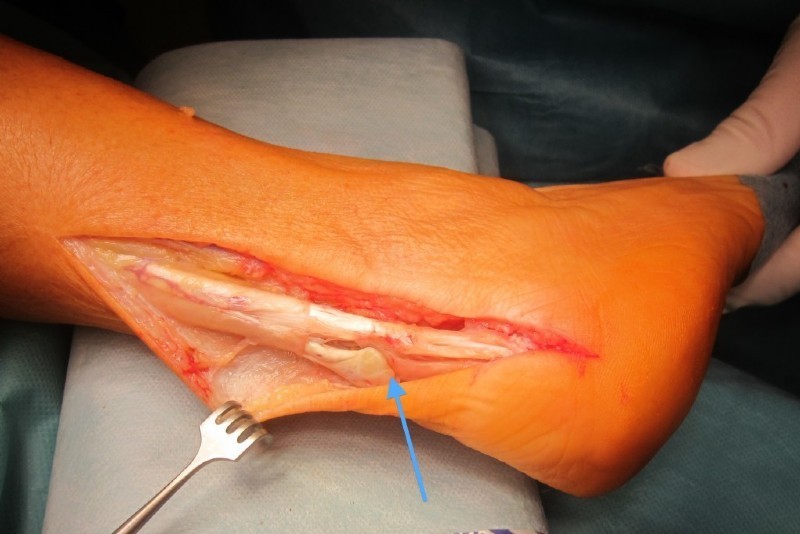

Left: More than half of the Achilles tendon is torn off along with the upper calcaneal spurs - arrow.
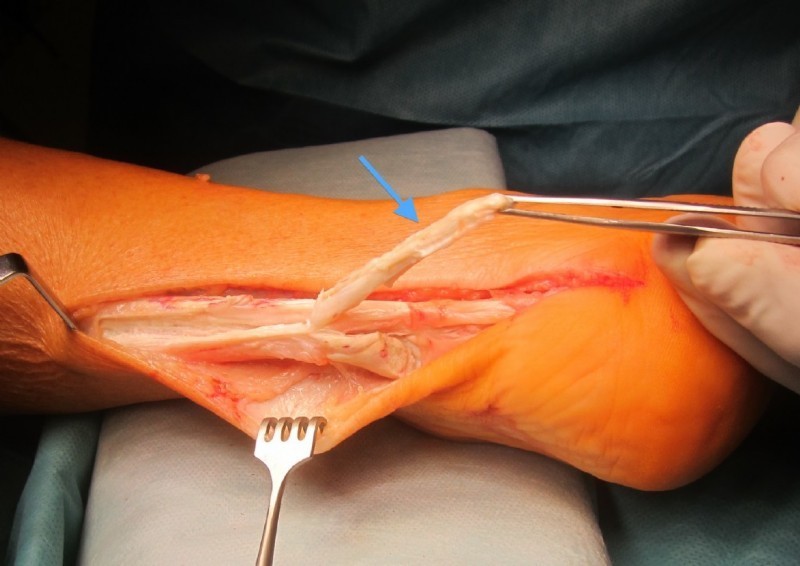
Middle: A so-called rotation plasty is formed. A piece of the tendon is folded under and sewn to the remaining tendon. In addition, a bone anchor made of plastic is used. The anchor is screwed into the heel bone and the Achilles tendon is also attached using its threads.
Right: The finished construction looks like an intact Achilles tendon.
Achilles heel afflictions
Achilles tendon inflammation, tendon sheath inflammation, tendonopathy
This disease is common in relation to underlying diseases such as gout, diabetes, and dyslipidemia, when overloaded by excessive activity or obesity and local blood circulation problems, and can affect the tendon itself (tendinitis, necrosis), the sheath (paratenonitis) or its enthesis (enthesitis).
Symptoms manifest themselves in the form of pain and a typical thickening of approximately 6 cm above the heel. The sheaths of the Achilles tendon become inflamed and later degenerate the tendon fibres themselves. Another common symptom is the so-called high heel bone (see below).
Treatment domains of this disease are conservative, with a plethora of options:
- tretching exercises
- cortisone-free infiltration
- physical measures
- medication
- shoe modifications
Special insoles are very effective in this case.
If these treatments fail, after a treatment period of approximately three months (except for tendon tears), surgery is opted for.
A longer waiting period would cause greater damage to the tendon and thus worsen the prognosis.
Treatment
If conservative treatment does not help, surgery is opted for, where necrosis (dead tendon parts) and inflammation are removed surgically from the tendon. This surgery is called combing because the inflammation of the tendon is actually combed out, so using small parallel cuts without substantial injury. Healthy tendon fibres are not injured and if enough fibres are still present, they must not be immobilized after surgery.
However, if there are knots and defects (necroses) in the tendon itself, then they are removed along with the tendon sheaths altogether.
If there are greater deficits in the tendon substance, then reinforcement measures must be taken, such as interlacing the tendon of the plantaris muscle. This is a thin tendon which extends parallel to the Achilles tendon. Reinforcement of large deficits or bridging in the case of total loss of substance is done with transplants, which are taken from the Achilles tendon itself (see fig.) Sometimes even a synthetic tendon must be used (see fig).
In the insertion of the tendon at the heel sometimes an ossification can sometimes develop (upper calcaneal spur), which leads to pain and inflammation, and must be removed. See there.
Post treatment
If only the tendon sheaths or bursa are removed, then subsequent treatment does not require a plaster cast. Physiotherapy early on is necessary to prevent a renewed adhesion. Even after "combing" immobilization is not a must., If enough tendon fibres are present,
If the operation required removal of more or less Achilles tendon substance,then a lower leg plaster cast must be worn for three to six weeks. In the case of large deficits or complete tears, which require a complete reconstruction of the Achilles tendon, a plaster cast must be worn for 8 to 12 weeks.
Ability to work
Office work can be resumed after about two weeks with a plaster cast, heavy physical work can be resumed two to four months depending on the prolongation of the operation.
Sports activities
Generally after six months, only in the case of minimal substance defect, earlier. This point should always be discussed with us.
Results
In over 90 percent of cases freedom of pain is attained or at least a significant improvement with good ability to function and do sports.
Complications
Infection under 2 percent, wound healing impairment or thromboses are rare.


Left: Chronic inflammation of the Achilles tendon, achyllodynia
Right: This Achilles tendon inflammation is highly acute. It occurred after a long hike, the chafing from hiking shoe can still be seen on the heel.
Achilles tendon ossification
Through constant friction of the Achilles tendon on a high heel bone, in particular when it is as sharp as in the example below, constant micro-cracks and bleeding occur. Sometimes the tendon tears partially or completely (see also chapter "High heel bone"). Sometimes bioremediation occurs in the form of bone growth in the Achilles tendon, as blood is a multipotent liquid from which almost all other tissue can develop.
Treatment
The ossification must be removed and the sharp upper heel bone corner must be levelled out. Afterwards, the amount of Achilles tendon tissue, which must be removed, can be seen. Reconstruction takes place either with own tissue or with a synthetic band – if too much tendon tissue had to be removed.
Post treatment
Plaster cast for 6 to 12 weeks, depending on the type and extent of reconstruction.
Ability to work and do sports
After the plaster cast is removed, intensive physiotherapy must be done for approximately 3 months. Heavy physical work and running are possible after 5 to 6 months after the operation.
Example:

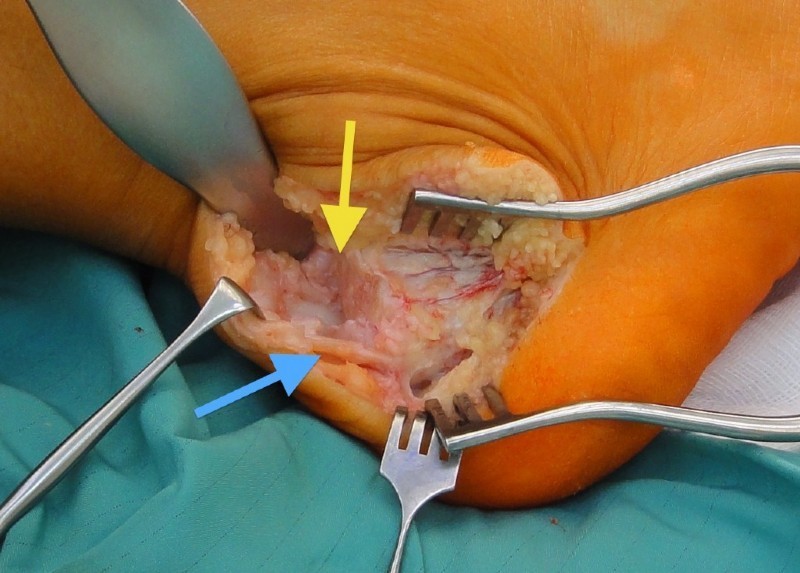
Left: Achilles tendon ossification- upper red arrow, sharp high heel bone – yellow arrow, additional lower calcaneal spur – lower red arrow
Middle: After removal of the ossification (blue arrow) and the high heel bone (yellow arrow)
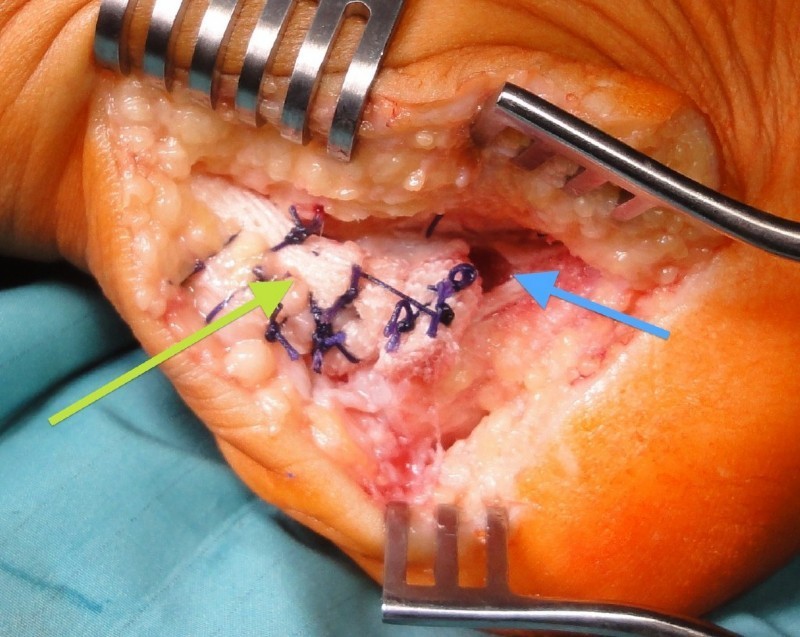
Right: Reconstruction of the Achilles tendon insertion on the heel bone with a synthetic band (Lars band), which is routed through a bone channel in the heel bone (blue arrow) and then sewn to itself and the Achilles tendon (green arrow).